 |
Browse by Strategy
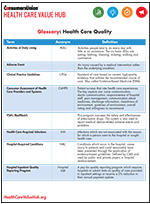
Quality Glossary Download
|
On this Topic
- Hub Webinar (April 2019)
Consumer-Centric Evaluation of Healthcare Price and Quality Transparency Tools - Hub Glossary
Healthcare Quality - United Hospital Fund
Empowering New Yorkers with Quality Measures They Value - Human Services Research Institute (June 2019)
Promoting Engagement on Healthcare Transparency Sites - Health Affairs (March 2012)
An Experiment Shows That a Well-Designed Report on Costs and Quality Can Help Consumers Choose High-Value Health Care
Improving Value
Publicly Reporting Quality Measures
Health disparities, medical harm and poorer health outcomes than other developed nations highlight the importance of quality improvement in creating a high-value and patient-centered health system.
Myriad strategies exist for improving population health, improving clinical outcomes and increasing patient satisfaction. One strategy is to leverage the power of publicly reported quality metrics to spur change.
Provider-facing Quality Transparency
Case studies suggest that, under the right circumstances, public reporting of quality metrics can lead to improvements in the quality of care that hospitals and clinicians provide.1 Hospital executives report that quality reports and hospital comparisons help focus their quality efforts.2 Evidence also suggests that individual clinicians and physician organizations respond to public reporting in positive ways, including by adding services, changing policy and increasing focus on clinical care.
Consumer-facing Quality Transparency
There is comparatively less evidence, however, supporting the claim that quality transparency affects patients’ choice of provider.3 As several researchers have pointed out, patients view healthcare quality differently than providers or quality measurement experts.4
Although clinical proficiency is important to consumers, most assume that healthcare providers are competent and their expertise is fairly uniform.
Additionally, patients often view quality in terms of the patient experience. Quality measures important to patients include the friendliness of office staff, listening skills of practitioners, length of wait times and cleanliness of the facility.
The mismatch between what is reported and what patients want to know contributes, along with other factors, to low use of publicly reported quality measures. Policymakers, regulators and payers require providers to report on a number of measures to protect consumers from insufficient quality. These include hospital-acquired infection rates, adherence to evidenced-based protocols and prevalence of “never events.” While important, these measures focus mainly on the technical and clinical aspects of quality that are difficult for consumers to understand. As a result, many quality transparency efforts fail to help people make informed decisions.
Contributing to this litany of barriers is low patient awareness of quality reports. A survey of chronically ill patients found that just 26% were aware of hospital quality reports and only 16% were aware of physician quality reports.5
Effective access and use of quality information requires that patients:6
- be aware of the information,
- understand the information being presented,
- find the information to be relevant to them,
- trust the source/are willing to act on the information, and
- receive the information in advance of making a decision.
Quality measures must meet people where they are in order to have the desired impact. A 2012 study in Health Affairs found that presenting quality information in consumer-friendly formats helped 90% of participants choose high-value care.7 Effective options included:
- Assigning providers one to three stars based on their ability to “prevent complications that could have been avoided”;
- Rating providers one to three stars based on their ability to “prevent complications that could have been avoided,” with a framing statement that said, “It is important to remember: With high-quality health care, many patient complications can be avoided;” and
- Assigning providers a “percent of patients with complications that could have been avoided and lower costs.”
According to many industry observers, despite “the dramatic growth in quality measures, public reporting and websites that display performance results,” these “are blunt tools, at best, for helping consumers find healthcare providers who match their needs.”8 Surveys show9 that consumers still rely on word-of-mouth recommendations from family, friends and their regular physician about individual clinicians, hospitals, post-acute care and long-term care.10
Barriers to Quality Reporting
Quality measurement is a relatively young science, and current measures are largely limited to what is easy to measure and validate. We find ourselves with an overwhelming number of quality measures in use, but also with a dearth of measures that resonate broadly with patients. Thus we need new measures that are proven to be trusted by consumers and help them make decisions, including those with low literacy and numeracy skills or limited English proficiency.
Quality measurement is also hindered by the surprising gaps in our comparative effectiveness research—for many of the healthcare services we receive, we simply don’t know if the treatment improves our health outcomes.
Finally, there are many organizations, both public and private, that currently have a role in designing, reviewing or collecting quality measures, and many other stakeholders who contribute to or use them. Inability to craft alignment across these stakeholders creates barriers to meaningful progress.
In Summary
Public reporting of quality measures—while more likely to be associated with changes in providers’ behavior than patients’—plays a key role in transforming our health system to one that is high-value and patient-centered.11 We should continue to use current measures that are working well, while designing new measures that are more patient-centered and better aligned across different stakeholders.
Notes:
1. Roland, Martin, and R. Adams Dudley, "How Financial and Rpeutational Incentives Can Be Used to Improve Medical Care," Health Services Research, Vol. 50, No. 2 (December 2015); Hibbard, Judith H., Jean Stockar and Martin Tusler, "Does Publicizing Hospital Performance Stimulate Quality Improvement Efforts?" Health Affairs, Vol. 22, No. 2 (March/April 2003).
2. Laschober, Mary, et al., "Hospital Response to Public Reporting of Quality Indicators," Health Care Finance Review, Vol. 28, No. 3 (Spring 2007).
3. Totten, Annette M., et al., Closing the Quality Gap: Revisiting the State of the Science (Vol. 5: Public Reporting as a Quality Improvement Strategy), Agency for Healthcare Research and Quality, Rockville, MD (July 2012).
4. For example, see: Rosen, Paul, "The Patient as Consumer and the Measurement of Bedside Manner," New England Journal of Medicine Catalyst, (March 20, 2017); University of Utah, First-Of-Its Kind Survey Reveals Significant Disconnects in How Three Key Stakeholders—Patients, Physicians, Employers—Perceive the Health Care Experience (Accessed June 30, 2017); McCarthy, Michael, "US Doctors are Judged More on Bedside Manner than Effectiveness of Care, Survey Finds," The BMJ, Vol. 349, No. g4864 (July 28, 2014); Public Values Research, 2017 Consumer Healthcare Priorities Study: What Patients and Doctors Want from the Health Care System, Pasadena, CA (2017).
5. Scanlon, Dennis P., et al., "Are Healthcare Quality 'Report Cards' Reaching Consumers? Awareness in the Chronically Ill Population," American Journal of Managed Care, Vol. 21, No. 3 (March 2015).
6. Maurer, Maureen, et al., "Understanding Consumer Perceptions and Awareness of Hospital-Based Maternity Care Quality Measures," Health Services Research, Vol. 51, Supplement 2 (February 2016).
7. Hibbard, Judith H., et al., "An Experiment Shows That a Well-Designed Report on Costs and Quality Can Help Consumers Choose High-Value Health Care," Health Affairs, Vol. 31, No. 3 (March 2012).
8. Rogut, Lynn B., "Searching for Quality Medical Care," Health Affairs Blog (Feb. 9, 2018).
9. The Associated Press-NORC Center for Public Affairs Research, Finding Quality Doctors: How Americans Evaluate Provider Quality in the United States: Research Highlights, Chicago, IL (July 2014).
10. U.S. Department of Health and Human Services, Assistant Secretary for Planning and Evaluation, Office of Disability, Aging and Long-Term Care Policy, Nursing Home Selection: How Do Consumers Choose? Volume I: Findings From Focus Groups of Consumers and Information Intermediaries, Washington, D.C. (December 2006).
11. Totten (July 2012).
HEALTHCARE VALUE HUB
The Healthcare Value Hub can help you find free, timely information about policies and practices to achieve health systems that are equitable, affordable, and focused on the goals and needs of the people the system is meant to serve.
Share
![]()
![]()
![]()

Follow
![]()
![]()


![]()