 |
Download
|
Policy Roadmap Toolkit
- Policy Roadmap - Main Report
- Appendix A: Policy Roadmap Summary
- Appendix B: Glossary of Terms
- Appendix C: Key Resources
- Appendix D: Key Federal Policies
- Appendix E: Key State Policies
- Appendix F: Crafting a Roadmap for Your Community: A Checklist
- Appendix G: 10 Places to Start
Consumer-Focused Health System Transformation:
What are the Policy Priorities?
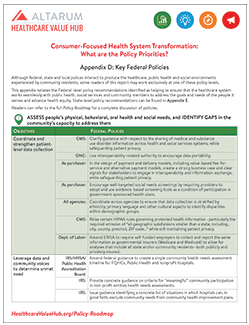
Appendix D: Key Federal Policies
Although federal, state and local polices interact to produce the healthcare, public health and social environments experienced by community residents, some readers of this report may work exclusively at one of these policy levels.
This appendix isolates the Federal-level policy recommendations identified as helping to ensure that the healthcare system works seamlessly with public health, social services and community members to address the goals and needs of the people it serves and advance health equity. State-level policy recommendations can be found in Appendix E.
Readers can refer to the full Policy Roadmap for a complete discussion of policies.
|
ASSESS people’s physical, behavioral, oral health and social needs, and IDENTIFY GAPS in the community’s capacity to address them |
|||||
|
OBJECTIVES |
FEDERAL POLICIES |
||||
|
Coordinate and strengthen patient-level data collection |
CMS: |
Clarify guidance with respect to the sharing of medical and substance use disorder information across health and social services systems, while safeguarding patient privacy. |
|||
|
ONC: |
Use interoperability-related authority to encourage data portability. |
||||
|
As purchaser: |
In the design of payment and delivery models, including value-based fee-for-service and alternative payment models, create a strong business case and clear signals for stakeholders to engage in interoperability and information exchange, while safeguarding patient privacy. |
||||
|
As purchaser: |
Encourage well-targeted social needs screenings by requiring providers to adopt and use evidence-based screening tools as a condition of participation in government-sponsored health plans. |
||||
|
All agencies: |
Coordinate across agencies to ensure that data collection is stratified by ethnicity, primary language and other cultural aspects to identify disparities within demographic groups. |
||||
|
CMS: |
Relax certain HIPAA rules governing protected health information—particularly the required omission of “all geographic subdivisions smaller than a state, including…city, county, precinct, ZIP code…” while still maintaining patient privacy. |
||||
|
Dept. of Labor: |
Amend ERISA to require self-funded employers to collect and report the same information as governmental insurers (Medicare and Medicaid) to allow for analyses that include all state and/or community residents—both publicly and privately insured. |
||||
|
Leverage data and community voices to determine unmet need |
IRS/HRSA/Public Health Accreditation Board: |
Amend federal guidance to create a single community health needs assessment timeline for FQHCs, Public Health and nonprofit hospitals. |
|||
|
IRS: |
Provide concrete guidance on criteria for “meaningful” community participation in non-profit entities health needs assessments. |
||||
|
IRS: |
Issue guidance identifying a concrete list of situations in which hospitals can, in good faith, exclude community needs from community health improvement plans. |
||||
|
Identify gaps in infrastructure, workforce, etc.
|
All Agencies: |
Facilitate information sharing across departments by developing standard processes for responding to data requests between departments and requiring that systems purchased to store data are capable of sharing it in multiple formats to aid in cross-departmental analyses. Consider making data available to the public and researchers. |
|||
|
HRSA: |
Ensure that federal data collection efforts that provide county-level information on the prevalence of medical professionals include professionals that address psychosocial needs, such as social and Community Health Workers. |
||||
|
CREATE INTEGRATED SYSTEMS to advance population health |
|||||
|
OBJECTIVES |
FEDERAL POLICIES |
||||
|
Align incentives to support population health goals |
CMS: |
Approve Section 1115 Delivery System Reform Incentive Payment (DSRIP) waivers to fund Accountable Communities for Health (ACHs). |
|||
|
All Agencies: |
Adopt cross-sector population health accountability measures to align incentives across vendor contracts (“parallel risk”). |
||||
|
Increase funding for services to address social needs |
CMS: |
Reactivate the Money Follows the Person (MFP) demonstration project. |
|||
|
Integrate healthcare and community-based services |
As Purchaser: |
Pay for care coordination activities under all types of provider payment models; couple these payments with outcome-based measures to ensure meaningful results; incentivize providers to use risk stratification or hotspotting to identify patients in need of coordinated care. |
|||
|
Engage community members in transformation efforts |
All Agencies: |
Have strong “open meetings” laws; hold meetings at times that are convenient for community members; assist with travel, childcare and translation services; and provide multiple avenues for public participation (online, in-person, etc.). Deploy principles of the Collective Impact Forum to ensure inclusiveness and impact. |
|||
|
All Agencies: |
Mandate consumer representation in health system governance whenever federal funds (or tax exemption) are used to provide services. Establish clear guidelines as to what constitutes sufficient consumer engagement. |
||||
|
ENSURE MEANINGFUL ACCESS to care and services that meet people’s goals and needs, especially within underserved communities |
|||||
|
OBJECTIVES |
FEDERAL POLICIES |
||||
|
Achieve universal, comprehensive coverage |
Congress: |
Pass comprehensive, universal health coverage legislation. |
|||
|
CMS: |
Alternatively, modernize the state flexibility offered under 1332 waivers to encourage all evidence-based coverage expansion approaches, while maintaining strict guardrails to ensure residents are not worse off. |
||||
|
AHRQ/NIH: |
Research to establish an evidence-based, fair “affordability standard” for healthcare. |
||||
|
Address provider shortages in underserved areas; increase diversity among providers |
HRSA/NIH: |
Increase loan repayment and scholarships to incent primary care, dental and behavioral health providers to serve in underserved areas of the country. |
|||
|
Increase the availability of Graduate Medical Education opportunities in rural and frontier areas. |
|||||
|
Tailor care delivery settings to community needs |
FCC: |
Restore subsidies that reimburse broadband providers for servicing rural areas. |
|||
|
Congress: |
Allow Critical Access Hospitals to offer primary care and telehealth services, as appropriate to meet the needs of community residents. |
||||
|
CMS: |
Permit demonstration projects to test new Critical Access Hospital based models of delivering care; broaden the scope of telemedicine services, settings and providers eligible for reimbursement under Medicare. |
||||
|
Make clinical care more patient-centered |
As Purchaser: |
Make shared decision-making as the standard of care, providing reimbursement, technical assistance with decision aids and an on-ramp that supports culture shift. |
|||
|
CMS/AHRQ/NIH: |
Support research on effective “anti-oppression and equity” trainings to prepare providers to operate in ways that combat structural racism and oppression. |
||||
|
Use measurement and feedback systems to judge performance |
HHS: |
Provide technical assistance, funding, and research to support to states and communities in identifying a core set of measures that reflect community priorities, to be used to assess overall system progress towards goals and establish a diversity of feedback mechanisms. |
|||
|
CMS/AHRQ/NIH: |
Prioritize the development and continued refinement of risk adjustment methods to account for social risk factors. |
||||
HEALTHCARE VALUE HUB
The Healthcare Value Hub can help you find free, timely information about policies and practices to achieve health systems that are equitable, affordable, and focused on the goals and needs of the people the system is meant to serve.
Share
![]()
![]()
![]()

Follow
![]()
![]()


![]()